Case study
A case of Hepatitis C
A senior citizen aged 79, the father of a close friend, was brought to me after detection of a Space Occupying Lesion (SOL) in the liver in June 2008. He was diagnosed has having a hepatocellular carcinoma by the imaging radiologist. He was a known case of HCV (detected positive in 1996). He had no symptoms suggestive of liver disease at the time.
The imaging report succinctly declared him to be the case of malignancy (hepat-ocellular carcinoma). The MRI report read like this:
There is presence of 3.2 x 3 cm size lesion hypointense on T1WI and hyperintense on T2WI images noted at junction right and left lobe superior aspect in segment IVA and VIII. On early arterial post-contrast study lesion shows intense enhancement and in portal phase it shows washout of contrast. On delayed phase peripheral capsule of lesion shows enhancement.
Rest of liver show does not show areas of altered signal intensity.
No dilatation of intrahepatic biliary radicles seen. Portal vein is normal in diameter.
There is presence of lobulated lesion which is hypointense on T1WI and hyperintense on T2WI in left paraaortic region just below left renal pedicle. The lesion measures 4 x 2.7 cm in size.
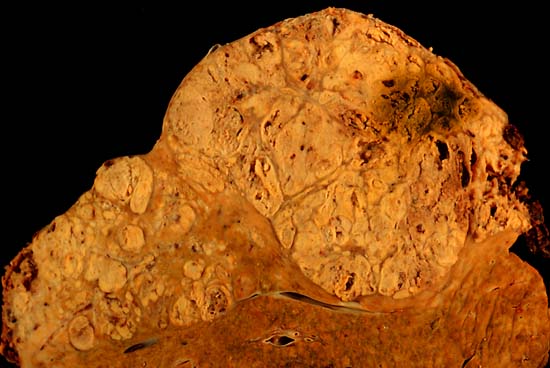
On USG the liver shows small multiple illdefined echogenic areas.
1. Overall findings suggest malignant lesion in liver at junction of right and left lobe superior aspect. Possibility of Hepatocellular carcinoma is likely. On Screening USG multiple echogenic areas may represent dysplastic nodules or small multiple focal hepatocellular carcinoma. Adv Biopsy for confirmation.
2. Possibility of paraganglioma in left para-aortic region just below left renal pedicle. However remote possibility of lymph nodes cannot be excluded.
The surgeons consulted advised immediate surgery. Every medical consultant was taking it for granted that he had a carcinoma with multiple secondaries. They explained the grave prognosis of the disease to the patient. They advised immediate surgery.
The patient’s son was eager to probe whether alternative therapies like homoeopathy could treat such a case. The patient’s ESR at the time was 33 mm/1st hour. We did not have earlier readings of the ESR.
I expressed doubt about the validity of the diagnosis of carcinoma based on an MRI report. Considering the fact that he had an active HCV infection and was 79 years of age, any surgical resection of a so-called malignant mass might have caused more morbidity than relief. Considering all this, we advised homoeopathic treatment with a review after a month. Keeping in mind the poor prognosis of a hepatocellular carcinoma in old age, one group of consultant physicians concurred with my advice.
The patient’s elder daughter, herself a doctor practising in the United States, was very keen on an instant surgical intervention “before it is too late”. After a lot of counselling, she too consented to homoeopathic treatment on a trial basis for one month. I suggested that we should not even take a biopsy as that itself might harm.
Clinical history
The patient had haemoptysis on waking up at 3.00 a.m. while travelling in a train in April 2008. It subsided immediately. The next morning he again woke up with haemoptysis. This induced him to undergo investigations which detected the masses in the liver.
Besides this, he had muscular pains in the lower extremities, especially on retiring to bed in the evening. This recovered after a sound sleep. In the mornings, he woke up absolutely refreshed. He was fresh in the mornings and better when occupied.
He had a history of constipation right from the age of 40 for which he used to regularly take laxatives.
His appetite was good. He always ate moderately and never too much. He liked sweets and salty food. His diet was strictly vegetarian. He used to develop acidity after consuming anything sour, especially sour buttermilk. He disliked anything sour as his teeth had become sensitive. He liked bland food.
His urine was clear.
His perspiration was moderate to scanty.
His sleep was sound and quick. He was most comfortable in the supine position or on either side. He had conspicuous dreams of a difficulty in finding a place for soiling.
He had a history of having fever at the age of 60 years, which was later treated as tuberculosis.
He was the fifth issue to his parents and had 7 siblings (two brothers and five sisters). He had been very active throughout his life. By nature he was bold and a fighter (kshatriya). He was very sensitive to insults. He could not tolerate injustice. However, he did not react impulsively. He waited for the proper time to react. He was very punctual in life. He followed the ideals of Gandhiji. Every day he relentlessly engaged himself in spinning cotton. Spinning was a daily meditation for him. He had leadership qualities. He had worked as a member of the Legislative Assembly for several consecutive terms and served as a minister for his home state. He was respected by all as a politician of high morals. He was elected also as a member of the Indian Parliament with a very successful tenure. He did not compromise on his principles while being active in politics. He was very hardworking and strict, but at the same time had a very loving nature. At times he used to feel suffocated in the changed scenario of politics. He took a keen interest in rural development and had been instrumental in the establishment of autonomous institutions to serve the rural population.
Past illnesses
Worm infestations were common when he was a child.
He developed glaucoma in both eyes in 1994 which was under control after regular treatment. His intraocular pressure was nearing 17 or 18 mm.
Both his eyes developed cataracts and subsequently they were operated upon. The right eye developed a cataract before the left. He had undergone surgery for a benign enlargement of the prostate as he had developed an interrupted flow of urine and subsequent retention of urine.
He had a mild history of jaundice in 1975 which was eventless. He was known to have carried an HCV infection over 15 years with esophageal varices and a fatty liver.
About Hepatitis C
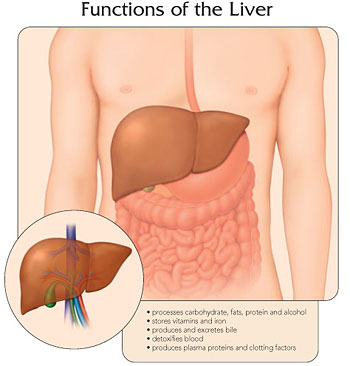
Hepatitis C is an infectious disease affecting the liver. It is caused by the hepatitis C virus (HCV) which is one of five known viruses (A, B, C, D, and E) affecting the liver. It was discovered in the 1970s and proved conclusively in 1989. It is one of the most frequent causes of chronic liver disease. An estimated 270-300 million people worldwide are infected with hepatitis C. It accounts for 60 to 70 percent of people with chronic hepatitis, and up to 50 percent of people having cirrhosis (end-stage liver disease) and liver cancer. Hepatitis C is the cause of about half of the cases of primary liver cancer in the developed world.
The infection is often asymptomatic, but once established, chronic infection can progress to scarring of the liver (fibrosis), and advanced scarring (cirrhosis) which is generally apparent only after many years. In some cases, those with cirrhosis go on to develop liver failure or other complications of cirrhosis, including liver cancer.
Acute hepatitis C refers to the first 6 months after infection with HCV. Chronic hepatitis C refers to infection of HCV persisting for more than six months. Clinically, it is often asymptomatic (without symptoms) and usually discovered accidentally. The factors that have been reported to influence the rate of HCV progression include age (increasing age associated with more rapid progression) and gender (males have more rapid disease progression than females).Can Hepatitis C be cured?
According to modern medicine, the only treatment for cirrhosis and liver cancer due to hepatitis C is a liver transplant but the virus generally recurs even after transplantation. There is no treatment in allopathy to eradicate hepatitis C . However, many patients do not develop any clinical disorders in their lifetime and remain carriers of Hepatitis C. One can perhaps conclude that if the immunity of the individual is good this infection can be contained at a sub-clinical level for the whole life.
The homoeopathic approach
The natural course of chronic hepatitis C varies considerably from one person to another. All people infected with HCV have evidence of inflammation on liver biopsy with consequent scarring (fibrosis) to variable degrees. The extent of damage to the economy of an infected individual varies according to the susceptibility of the individual. Homoeopathy aims at improving the host immunity to control the progress of the infection and minimise its long-term complications. Homoeopathy has many remedies which can specifically make the liver and allied organs healthier. There are a host of plant remedies which have a specific affinity for the liver and allied organs.
Homoeopathic medicines are proved on healthy human beings (not animals) in order to know their pure properties in human beings. They have been known to avert complications arising after HCV infection.
Considering the above facts, in this case we decided to give organ remedies or tissue remedies in lower dilutions from June 4, 2008.
He was given a single dose of Carcinocin 1M followed by Chelidonium 3X, Carduus mariannus 2X, Hydrastis can 2X , Chionanthus 3X in drop doses (ten drops bd in half a cup of water) and Thuja 6C tds over two weeks. After a month the MRI report indicated that the mass was status quo. The para-aortic lymphatic mass had receded to some extent. We decided to wait and watch the response to homoeopathy. The same course of Chelidonium 3X, Carduus mariannus 2X, Hydrastis can 2X , Chionanthus 3X in drop doses (ten drops bd in half cup of water) was continued. The MRI on October 31, 2008 revealed that the mass had receded to some extent.
We went on giving Chelidonium 3X, Carduus mariannus 2X, Hydrastis can 2X , Chionanthus 3X in drop doses (ten drops bd in half cup of water) for 8 months and the various readings are as shown in the tables.
ESR readings
Date |
ESR |
10-Jun-08 |
31 mm/1hr |
23-Jun-08 |
40mm/1hr |
16-Oct-08 |
37mm/1hr |
18-Dec-08 |
35mm/1hr |
6-May-09 |
32mm/1hr |
23-Jun-09 |
15mm/1hr |
22-Sep-09 |
5mm/1hr |
Viral Load Readings
| Date |
HCV RNA(BY ROTOR GENE - 3000 Calc conc. Copies) |
| Jan 31, 2009 |
3980 |
June 24, 2009 |
2860 |
The liver functions tests
DATE |
Protein-T (6.6 to 8.7gm/dl) |
Albunin (4.0-5.5 gm/dl) |
Globulin (2.3-3.5gm/dl) |
Sgot (up to 50 U/L) |
Sgpt (up to 50 U/L) |
30 Apr-08 |
124 |
95 |
|||
23 May-08 |
7.19 |
3.69 |
3.5 |
104 |
|
23 Jun-08 |
7.50 |
3.90 |
3.6 |
92 |
48 |
6 Aug-08 |
75 |
47 |
|||
16 Oct-08 |
7.30 |
3.90 |
3.4 |
65 |
43 |
18 Dec-08 |
7.50 |
4.40 |
3.1 |
63 |
41 |
23 Jun-09 |
6.80 |
3.70 |
3.1 |
31.5 |
43.1 |
MRI readings of the hepatocellular mass
Date |
Size of malignant lesion |
Size of Para-aortic Lymph node |
31 May-08 |
32 X 30 mm |
40 X 27 mm |
4 Jul-08 |
31 X 27 mm |
30 X 26 mm |
25 Aug-08 |
31 X 28 mm |
30 X 26 mm |
31 Oct-08 |
33 X 30 mm |
30 X 26 mm |
30 Jan-09 |
34 X 28 mm |
36 X 23 mm |
9 May-09 |
36 X 27 mm |
37 X 24 mm |
Conclusion
The above reports clearly indicated that there is no active liver pathology. The consistent reversal of ESR indicates that the chronic pathological conditions have reversed. The viral load of HCV has considerably come down indicating a decline of Hepatitis C virulence. The liver functions have also recovered. The so-called malignant lesions of hepatocellular carcinoma have not progressed at all in one year and even the para-aortic lymph node has regressed.
Follow-up
We are now observing this person without remedies, taking into account the behaviour of HCV infections. HCV infections are supposed to progress quickly among males and especially aged ones. The patient’s treatment with tissue remedies has been stopped as he is asymptomatic. We definitely intend to monitor him for a longer period till we find HCV RNA are down to undetectable levels.
Share with us (Comments, contributions, opinions)
When reproducing this feature, please credit NAMAH, and give the byline. Please send us cuttings.